
What is Bio Leadership in the 21st Century?
Policy, Funding, and Technology in the New Era of Pharma
The United States still leads the world in biotechnology. But leadership is not a law of nature. It is the product of policy, capital allocation, regulatory philosophy, and operational execution.
If we want to understand how America maintains or loses its edge to China and others, we need a clear framework. I think about US biotech leadership across four levers:
Science
Commercial
Regulatory
Operational
Each lever has subcomponents. Each can either compound the U.S. advantage or quietly erode it.
Below is how I see the system and where policy and technology can make the biggest difference.
Preclinical Science: The Foundation

Panoptic Bio is a pharma intelligence company in Mountain View, CA
The American biotech advantage starts in universities.
The U.S. system of government funded preclinical research, primarily through NIH, NSF, SBIR, and related programs, has no true peer. Add to that DARPA, ARPA H, and defense linked funding streams, and you have a deep reservoir of early stage discovery science.
This is not an accident. It is a policy choice.
Preclinical science is hard to fully privatize. The timelines are long. The failure rates are high. The ROI is uncertain. Venture capital does not fund decades long fundamental biology programs without a translational hook.
Later stage development can be privatized. Early stage science cannot be fully privatized without hollowing out the pipeline.
If the United States cuts government science funding, it is not trimming fat. It is weakening the root system of its pharmaceutical tree.
China understands this. It is massively expanding state backed fundamental research. If the U.S. cuts while China expands, the long term consequence is obvious.

The U.S. and China are in a strategic competition with areas of collaboration to advance biotechnology and pharma innovation, deciding who will lead in the 21st Century.
It is critical the U.S. and Europe preserve and expand federal funding for preclinical science.
If politically difficult, there is a second path.
The U.S. should treat biotech as national security.
Public health is national security. Healthy civilians and healthy soldiers are strategic assets. Biosecurity is a dual use domain. Just as climate was once framed as a defense issue, biotechnology should be embedded more deeply into defense budgets.
If civilian science funding contracts, defense aligned funding should expand to compensate. The Military can play a larger role in sustaining American bio innovation capacity through its funding vehicles.
Immigration policy also matters here. The US academic system attracts global talent. If funding shrinks and visas tighten, the U.S. will hollow out its own preclinical advantage.
Preclinical science is not optional. It is the seed corn.
Clinical Stage Science & Capital Markets
Once assets move into the clinic, the funding structure changes.
Here the United States has a powerful advantage: capital markets.
VC. Growth equity. Private equity. IPO markets. Follow on offerings. Private placements. Structured credit. Pharma partnerships.
The US has deep, risk tolerant capital pools that fund clinical development at scale. China has capital, but it does not have the same depth of global commercial opportunity or exit liquidity.
But capital allocation matters.
The U.S. should not only fund therapeutic assets. The U.S. should fund infrastructure:
AI enabled drug discovery platforms
Genetic and multiomics infrastructure
Trial technology
Data platforms
Manufacturing innovation
Private capital should increasingly flow into the infrastructure that accelerates all future therapeutics, not only the next molecule.
Commercial: Pricing and Global Fairness
The commercial lever is about pricing and incentives.
The United States currently supports biotech innovation through high domestic pricing. US patients often pay two to ten times what patients in Europe pay for the same drug.
In practice, America subsidizes global innovation.
Other countries regulate pricing tightly. They wait for US funded innovation and then negotiate aggressively. This is a form of pharmaceutical protectionism.
If the US maintains high pricing domestically but does not push for market openness abroad, American patients shoulder disproportionate burden.
The answer is not simply to crush US pricing. That would damage innovation incentives.
The better path has two components:
Preserve domestic pricing incentives that sustain ROI.
Pressure international markets to open access.
Most favored nation pricing proposals are politically attractive. But if applied without higher foreign pricing, they effectively import low price regimes into the US and compress global innovation margins.
If we want fairness, we must address global pricing asymmetry, not only domestic optics.
Rebates and Trial Location Arbitrage
Commercial policy also affects where trials happen.
US clinical trials are extraordinarily expensive. CRO dominated infrastructure, administrative burden, and site costs push per patient costs into six figures in some indications.
In contrast:
China can run trials at a fraction of the cost.
Australia offers substantial government rebates, sometimes around 40 percent.
Other jurisdictions aggressively compete for clinical trial flow.
If the US wants to reshore trials, it needs incentives. Rebates tied to domestic clinical trial spending could bring trials back onshore.
Otherwise, rational companies will continue to run pivotal programs abroad and bridge into the US later.
Regulatory: Safety, Speed, and Statistical Innovation
The FDA, EMA, and NMPA represent three major regulatory centers of gravity.
Historically, the FDA has been the most rigorous and often the most difficult to navigate. In many therapeutic areas, sponsors perceive it as more conservative than the EMA. The NMPA has been less rigorous historically but is increasing standards.
Regulatory stringency is not inherently bad. Safety matters. But overregulation can silently cost lives through delayed approvals.
We need an honest conversation:
How many lives has the FDA saved by not approving unsafe drugs?
How many lives has been lost because beneficial drugs were delayed or never approved?
We do not measure the second number clearly. That is a policy blind spot.
Reforms worth expanding include:
Acceptance of a single pivotal trial in certain oncology settings.
Greater use of real world evidence.
Broader adoption of Bayesian statistical methods in SAP design.
Adaptive and accelerated pathways that balance uncertainty with urgency.
The regulatory goal should not be deregulation for its own sake. It should be optimized risk balancing.
We must balance patient safety today with patient health tomorrow.
If Europe is easier to get through than the United States, and if China continues accelerating its pathways, the US risks becoming the slowest node in the global innovation chain.
That is not compatible with leadership.
Operational: Trials, Data, and Infrastructure
This is where much of the hidden inefficiency lives.
Clinical Trial Cost Structure
CROs dominate the current system. Trials are centralized. Sites are dependent. Administrative overhead is immense.
Enrollment delays kill companies. Companies run out of runway because recruitment lags.
There is another model.
Decentralize trials.
Physician led trials
Professor led academic trials
Enabling community clinics as sites
Reducing dependence on centralized CRO control
In China, physician autonomy in trial participation is broader. If every qualified physician office in the US could more easily function as a trial site, enrollment velocity would increase dramatically.
We need infrastructure that lowers friction to becoming a site.
Heterogeneous Populations as Strategic Advantage
The US population is heterogeneous. That is an advantage.
Chinese data often requires bridging studies before being accepted in Western markets because of population homogeneity concerns.
US trials, if designed with broad inclusion criteria and heterogeneous enrollment, can generate globally generalizable data.
We should codify heterogeneous representation requirements not as ideology but as global competitiveness strategy.
If American trials reflect the world, American drugs become global by default.
Data Infrastructure: Fragmented vs Unified
China benefits from unified medical data infrastructure. It can query large portions of national health data, identify rare disease patients, and accelerate enrollment.
The United States has:
Fragmented EHR systems
State level legal variation
Privacy complexity
Limited interoperability
Barriers to large scale model training
We cannot ignore this.
Unified does not mean unsafe. Encrypted, privacy preserving, federated architectures can enable large scale AI without exposing raw data.
But if we do not build national scale health data infrastructure:
Patient to site matching remains inefficient.
Rare disease identification remains slow.
Trial recruitment remains costly.
AI models remain underpowered.
Data is the substrate of modern biotech.
Clinical Trial Intelligence and Workflow Automation
The next frontier is workflow automation across the entire biotech lifecycle.
Signal capture and due diligence
Patient matching and enrollment
Dosing and follow up
Manufacturing and CMC
Quality control
Regulatory documentation
Commercial launch
Marketing
Every one of these is a workflow problem.
Clinical trial intelligence means:
Automating patient identification across EHR systems.
Automating eligibility checks against inclusion and exclusion criteria.
Automating site activation.
Automating data monitoring.
Automating safety signal detection.
Automating CMC documentation.
Automating market access analytics.
This is not only cost reduction. It is speed. And speed saves lives.
If AI is trained on large scale, well structured, interoperable health data, the US can create a compounding advantage in development velocity.
If we fail to modernize data infrastructure, others will.
The Strategic Picture
Across science, commercial, regulatory, and operational levers, the pattern is clear:
Expand and protect preclinical government funding.
Leverage defense budgets for biosecurity and dual use biotech.
Preserve domestic pricing incentives while pushing for international fairness.
Modernize regulatory pathways with adaptive and Bayesian methods.
Reduce trial costs through decentralization and site empowerment.
Build unified, privacy preserving health data infrastructure
Invest in clinical trial intelligence and workflow automation.
Biotech leadership is not a single policy decision. It is a systems outcome.
China is a gift to the United States. In the sense that competition is exactly the urgency the pharmaceutical industry needs to wake up and become more efficient.
Clinical Trial Intelligence plays a key role in this drive towards greater efficiency.
Clinical trial intelligence is the integrated, AI driven layer that sits across the entire clinical development process, structuring fragmented data into a unified model of trial risk and decision making. It pulls together scientific rationale, protocol design, regulatory precedent, operational performance, competitive landscape, CMC readiness, and commercial viability into a single probabilistic framework. Instead of leaving these domains siloed across PDFs and functional teams, clinical trial intelligence transforms them into a structured system that benchmarks against historical programs, runs counterfactual scenarios, and identifies where failure is most likely to emerge before it happens.
Why Panoptic Bio Exists
This is the gap Panoptic Bio addresses.
If efficiency is the constraint, and Phase I to approval remains a roughly 7.9 percent outcome over more than a decade, the biggest leverage is not marginally better discovery. It is a better clinical-stage decision system.
Faster decision cycles. Higher-quality evidence synthesis. Greater consistency. Scalable learning across programs.
Clinical trials should not be driven by fragmented, manual intelligence. They should be guided by systems that learn continuously from trial reality and translate that learning into better decisions and better execution.
This is where failure is most expensive. It is also where decision intelligence matters most.
If China’s advantage is execution throughput, the Western response must be decision superiority paired with execution strength. That means building a modern pharma operating system that converts AI leadership into sustained biotech leadership.
Panoptic Bio’s Trial Terminal is a decision intelligence platform to safely run AI models and agents on ongoing clinical trials
Retrieve any registered clinical trial from the U.S., Europe, China, or globally
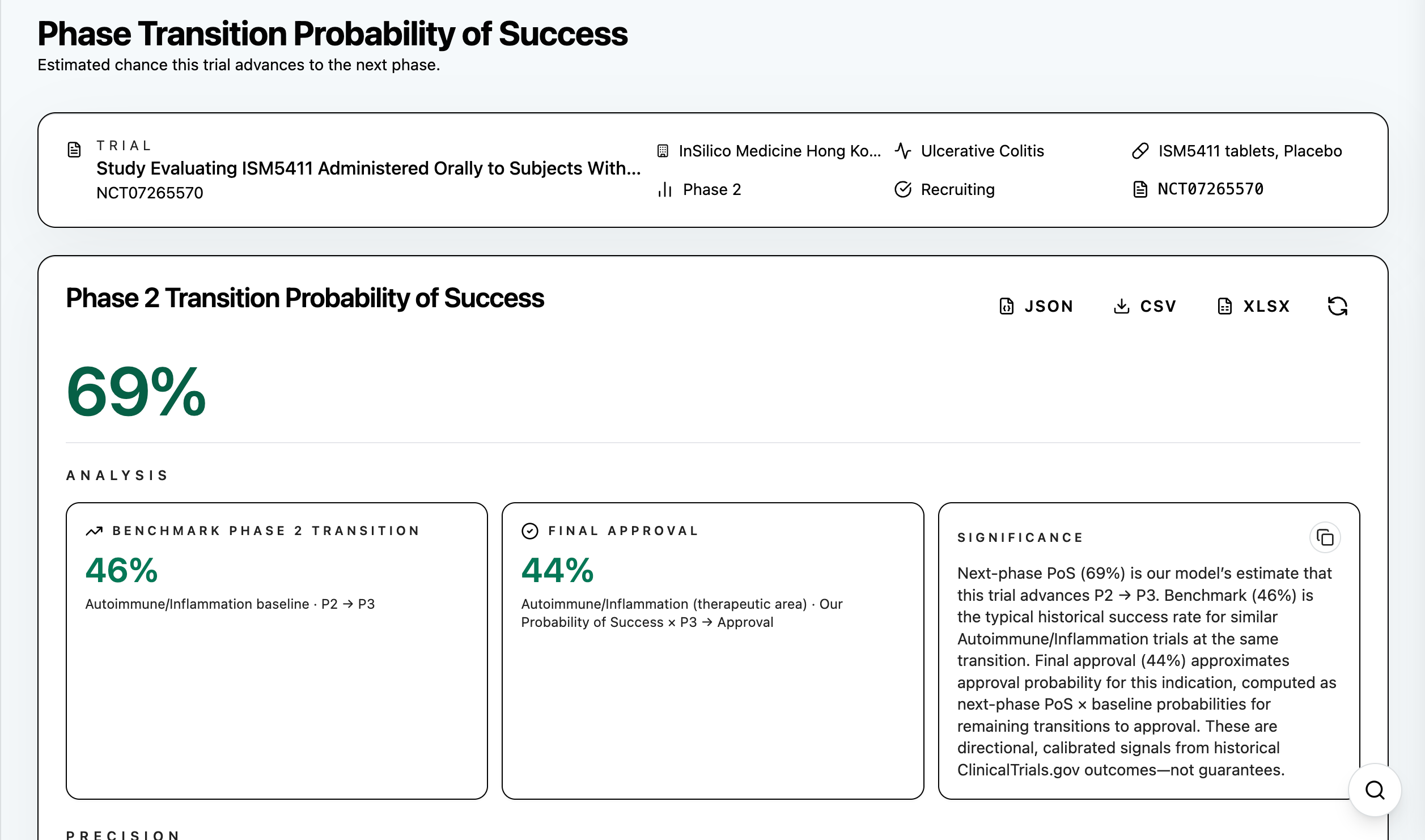
Run Probability of Success analysis on ongoing clinical trials
Who will lead the 21st century?
The importance of clinical trial intelligence lies in addressing the real bottleneck in pharma, which is not molecule discovery but the 92 percent failure rate in clinical development. Even strong biology fails when one weak dimension cascades across the system. By quantifying risk, forecasting outcomes, and recommending targeted interventions at the design stage before millions are spent, clinical trial intelligence increases the probability that programs reach approval. Even a one percent improvement in success rates translates into enormous economic value and, more importantly, more therapies reaching patients. In this model, clinical trial intelligence becomes the infrastructure layer of an AI native pharma stack, determining which discoveries ultimately become medicines.
In the end, biotech leadership will not be decided solely by who discovers the most novel targets, but by who builds the fastest and most intelligent development system. The United States still leads in science and AI, but without upgrading its decision infrastructure, that advantage will dissipate into inefficiency. China’s rise demonstrates that execution throughput compounds into strategic leverage. The next era of pharma will be defined by integrated decision intelligence that shortens learning cycles, improves capital allocation, and increases the probability that the right programs reach patients. Sovereignty, competitiveness, and patient impact now hinge on who builds the better decision loop. Bio leadership in the 21st century belongs to those who deploy clinical trial intelligence.
