how to launch your own agent-run pharma company
hello and welcome to the future of pharma. machines make medicine now. here’s how you launch one.
For the last hundred years, starting a pharma company meant doing something almost absurdly hard. You found a molecule, raised a lot of money, hired scientists, outsourced experiments, waited, ran studies, waited again, wrote regulatory documents, waited more, and then maybe, if biology was kind and the trial worked and the factory could make the drug, you got a medicine.
10 years and $1B+ spent.
Maybe.
This old playbook worked 8% of the time.
It gave us antibiotics, vaccines, statins, antibodies, GLP-1s, cancer immunotherapies, antivirals, and rare-disease drugs. Modern medicine is a miracle. But the machine that creates it is slow, expensive, fragmented, and full of handoffs.
This is not because pharma is dumb. It is because pharma is hard. Biology is hard. Patients are different from each other. Clinical trials are expensive. Manufacturing is regulated. Quality matters. Regulators are cautious because they should be. The body is not software. You cannot ship a broken update into a human being.
But the company structure is also broken. Pharma is not one business. It is ten businesses wearing a lab coat. A pharma company has to discover drugs, test safety, design trials, recruit patients, collect data, manufacture medicine, handle quality, work with regulators, get paid by insurers, educate doctors, and monitor safety after launch. Historically, all of this has been split across vendors, consultants, spreadsheets, databases, hospitals, contract manufacturers, and internal teams.
Every handoff adds time. Every handoff adds cost. Every handoff adds error. Every handoff loses information.
The next great pharma company will not be a better version of this old machine. It will be a new machine: an AI-native pharma company.

By AI, I mean software that can read, reason, predict, draft, search, and help make decisions. By AI-native, I do not mean adding a chatbot to an old pharma workflow. I mean building the whole company around artificial intelligence from the beginning. AI proposes. Software executes. Robots run experiments. Simulations prioritize. Humans approve the high-risk decisions. Regulators receive a clear record of what happened and why.
That is the new playbook.
The first thing you build is not a molecule. The first thing you build is memory.
Memory
A pharma company is only as good as what it remembers: every paper, every failed trial, every assay, every patient group, every biomarker, every dose change, every protocol amendment, every safety issue, every manufacturing batch, every payer objection, every label update. Traditional pharma stores this memory in people, PDFs, email threads, folders, outsourced vendors, and institutional lore. The AI-native pharma company stores it in a scientific memory: one connected system that learns from every molecule, trial, patient, batch, launch, and safety signal.
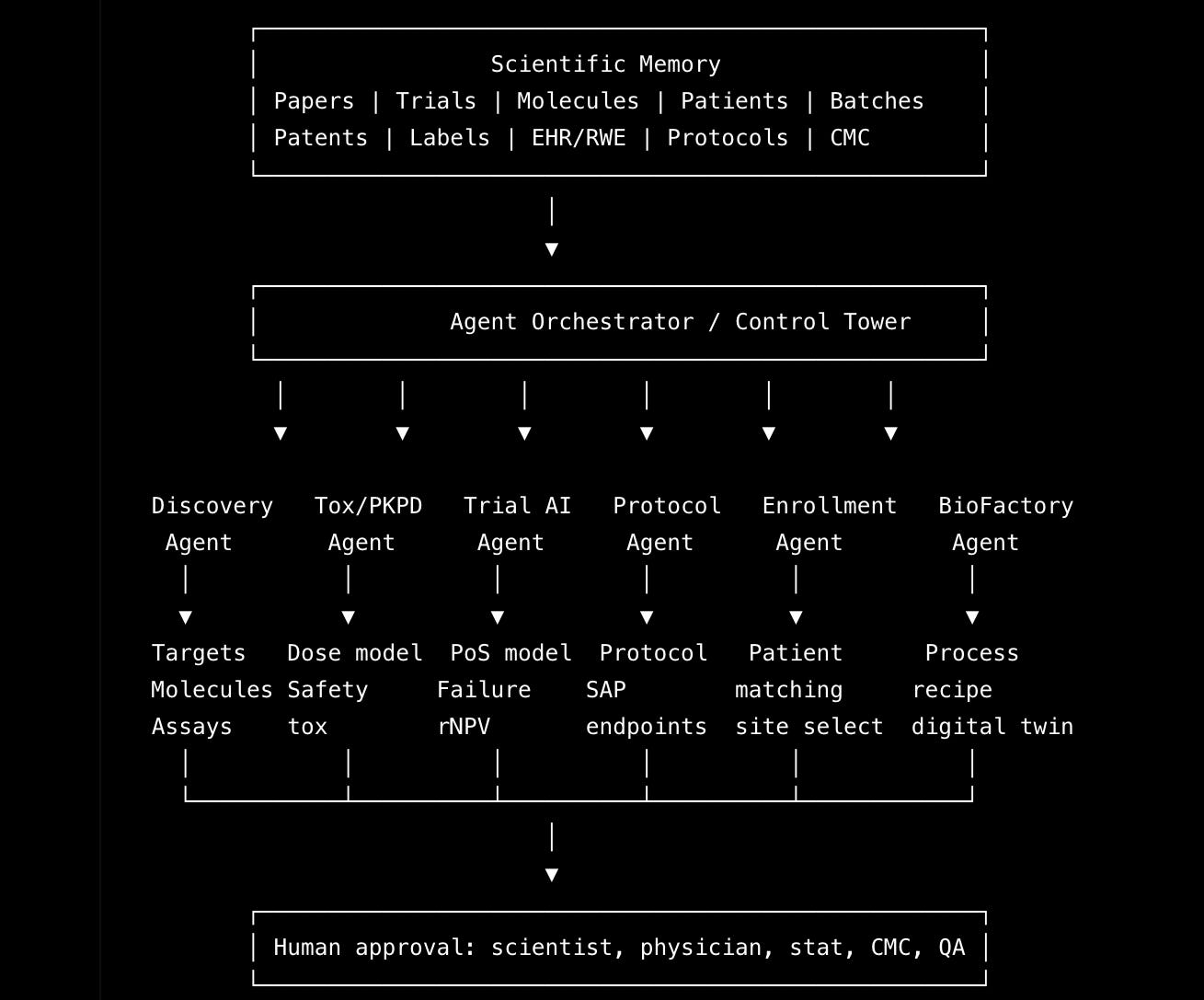
This scientific memory becomes the company’s brain. The discovery system uses it to find drug ideas. The safety system uses it to predict risk. The trial system uses it to decide whether a drug is likely to work. The enrollment system uses it to find patients. The manufacturing system uses it to make the drug. The launch system uses it to understand the market. The quality system watches everything. This is the basic architecture of the vertically integrated AI-native pharma company: one memory, many specialized agents, and humans approving the decisions where safety and accountability matter.
But you do not build the whole thing on day one. That is how you die.
The smallest credible version starts with clinical trial intelligence. Clinical trial intelligence means understanding which drugs are likely to succeed in human trials and why.

This is the best place to start because the data already exists. There are public trial registries, medical papers, drug labels, patents, press releases, conference abstracts, regulatory documents, and years of failed and successful trials.
You do not need a wet lab to begin. You do not need a factory to begin. You do not need 500 people to begin. You need a system that can answer one question better than everyone else: will this drug work?
Not “is the science interesting?” Not “does the pitch deck look good?”
Will this drug work in this disease, in this patient population, at this dose, against this comparator, with this endpoint, under this regulatory path?
This is where the company begins. Not with a molecule. With judgment.
The first product should feel like Bloomberg Terminal for drugs. Panoptic Bio calls it the Trial Terminal.
A clinical asset goes in, and a decision comes out. The input is a drug, target, disease, trial, or company. The output is a complete map: what the drug does, what failed before, what worked before, which patients matter, which endpoints are credible, which competitors are ahead, which trial design makes sense, what the risks are, and whether the asset is worth buying, licensing, redesigning, or killing.
A human analyst can do this slowly. A great team can do this expensively. An AI-native pharma company should do this continuously.
AI drug rescue.
The first AI-native pharma companies do not need to invent every drug from scratch. They can buy mistakes. Pharma creates mistakes constantly. Good molecules are tested in the wrong disease. Good mechanisms are tested in the wrong patients. Good assets are killed after underpowered trials. Good drugs fail because the endpoint was wrong. Good programs get stuck because manufacturing was messy or enrollment was too slow.
The opportunity is to find the asset everyone else thinks is dead and ask why it died. Was it biology? Was it dose? Was it endpoint? Was it patient selection? Was it manufacturing? Was it commercial? Or was it simply owned by the wrong company at the wrong time?
Then you produce the only memo that matters: here is the asset, here is why it failed, here is why we think it can work, here is the redesigned trial, and here is the probability that we are wrong.
That is a pharma company.
Protocols
Once you know the asset, you need the trial. This is where old pharma becomes obviously insane. A clinical protocol is one of the most important documents in medicine. A protocol is the master plan for a clinical trial. It defines who can join, what dose they get, what doctors measure, how safety is monitored, how often patients visit, what counts as success, and what regulators will review.
And yet protocols are often written like legal documents passed through a committee of 47 people who each add risk but not clarity.
The AI-native pharma company builds a Protocol Machine. The Protocol Machine turns an asset strategy into a trial plan. It studies similar successful and failed trials. It asks which patient criteria slowed enrollment, which endpoints regulators accepted, which amendments happened later and should have been obvious earlier, and which design choices created unnecessary burden for patients.
The AI system writes the first draft. The statistician checks the math. The physician checks the medicine. The regulatory lead checks the rules. The operations team checks whether the trial can actually run. Then humans approve it.
That pattern matters: AI drafts, AI simulates, AI stress-tests, humans approve.
AI-native does not mean AI-only. Especially not in medicine. The future is not autonomous agents secretly dosing patients and releasing drugs. That is science fiction and also a nightmare. The future is a company where AI compresses the work, expands the search space, catches mistakes, keeps the evidence trail, and makes expert humans dramatically more effective.
Enrollment
The next task is enrollment. A trial without patients is not a trial. It is a PDF.
Clinical trials often fail slowly because they cannot find enough eligible patients at the right sites at the right time. The old way is site surveys, investigator relationships, optimistic spreadsheets, manual chart review, and prayer.
The AI-native way is patient-trial matching. The trial criteria become computable. The system looks across approved medical data sources and identifies which hospitals are likely to have eligible patients. It estimates screen failure, meaning how many patients appear eligible at first but fail once fully reviewed. It flags competing trials. It predicts enrollment speed. It helps coordinators find likely matches.
But it does not bypass ethics. Patients are not ad targets. A site investigator and coordinator still approve contact. Patients still consent. Doctors still make the final eligibility decision.
The company that controls enrollment intelligence controls clinical speed. And speed in pharma is life.
Making the medicine
After digital AI comes physical AI. Digital AI is software that reasons. Physical AI is software connected to robots, sensors, lab equipment, and manufacturing systems. This is where the next pharma company becomes very different from a software company.
Software can find the drug. Software can design the trial. Software can match the patient. But at some point, atoms matter. You have to make the medicine at clinical grade, under regulation, reliably, repeatedly, and at scale.
This is where the current system breaks again. Clinical development and manufacturing are treated like separate worlds. They are not. They are one loop.
The trial tells you what dose you need. The dose tells you how much drug you need. The formulation affects whether patients take it correctly. The manufacturing process affects purity. Purity affects safety. Safety affects dose. Dose affects efficacy. Efficacy affects trial design. Trial design affects manufacturing demand.
Manufacturing is not downstream of clinical development. Manufacturing is part of clinical development.
Eventually, the AI-native pharma company needs a BioFactory OS. OS means operating system: the control layer that coordinates the work. A BioFactory OS connects process development, sensors, batch records, quality checks, release testing, supply planning, and automated manufacturing. It watches the process in real time. It predicts when a batch may fail. It recommends adjustments. It flags deviations. It prepares quality review.
But it never releases medicine without human approval. Quality assurance still matters. Regulators still matter. Human accountability still matters.
This is the bridge from digital AI to physical AI. Machines do not just discover medicine. Machines make medicine. Clinical trials and manufacturing are not separate systems. They are one loop, and the next company should connect them directly.
Taking medicine to patients!
Most biotech founders think the story ends at approval. It does not. Approval is when the second company begins.
Now you need market access, meaning the work required to get insurers and health systems to pay for the drug. You need medical affairs, meaning the team that communicates scientific evidence to doctors and researchers. You need pharmacovigilance, meaning post-market safety monitoring. You need supply, distribution, adherence, real-world evidence, and label expansion.
Real-world evidence means evidence from actual clinical use after approval: claims, prescriptions, lab results, registries, doctor notes, and patient outcomes. The AI-native pharma company treats the market as the next learning loop. Every prescription, claim, safety report, refill, discontinuation, physician question, payer objection, and patient outcome teaches the system something.
Traditional pharma runs a trial, launches a drug, and then collects post-market data because it has to. AI-native pharma launches the drug and keeps learning because that is the whole point.
So how do you actually launch?
First, build the Trial Intelligence and Due Diligence Engine. Use public and licensed data. Analyze active and failed trials in one therapeutic area. Predict probability of success. Diagnose failure modes. Write asset memos. Find mispriced drugs.
Second, acquire or license one drug. Not ten. One. The best first asset is not the flashiest asset. It is the one where the failure mode is fixable: wrong endpoint, wrong patient population, wrong dose, poor enrollment, bad trial design, or a manufacturing issue you can solve.
Third, redesign the trial. Make the protocol computable from the start. Use AI to draft, simulate, and stress-test. Use humans to approve. Meet regulators early. Design the trial so the machine can help run it.
Fourth, build enrollment infrastructure. Partner with sites. Map patients compliantly. Reduce screen failure. Track bottlenecks in real time. Make enrollment an operating system, not a weekly meeting.
Fifth, connect manufacturing. At first, partner with manufacturers. Then automate process development for one type of medicine. Do not build a factory for everything. Pick one modality, meaning one category of medicine, such as antibodies, small molecules, recombinant proteins, mRNA medicines, viral vectors, or cell therapies. Instrument everything. Make every batch teach the system.
Sixth, launch with real-world evidence from day one. Market access is not a deck. Medical affairs is not a call center. Safety monitoring is not paperwork. They are all part of the learning loop.
The first team does not need to look like a classic pharma org chart. You need a small team that can cross software, biology, medicine, regulation, and operations. You need a founder who can raise money and hold the whole system in their head. You need a clinical development lead, a physician-scientist, a regulatory lead, a machine-learning lead, a data-infrastructure lead, a product engineer, a business-development lead, a manufacturing advisor, and a quality-minded operator who understands that pharma is not SaaS.
A lot of companies want to sell SaaS tools to pharma. That is fine. But the bigger opportunity is not to sell dashboards to the old system. The bigger opportunity is to become the new system.
machines that make medicine
The next great pharma company will look like a self-driving machine. It will have a brain that reads every paper, trial, label, protocol, patent, safety report, and batch record. It will have AI agents that reason across discovery, safety, clinical development, enrollment, manufacturing, regulation, and launch. It will have robots and sensors that make biology measurable and manufacturing repeatable. It will have humans at the gates where judgment, ethics, safety, and accountability matter.
The old pharma company asks: can we discover a molecule?
The new pharma company asks: can we build a machine that continuously discovers, tests, manufactures, launches, and learns from medicine?
That is how you launch your own pharma company. Not by starting with a drug, but by starting with the loop.
Hypothesis → AI design → simulation → robotic experiment → evidence update → human approval → trial → manufacturing → launch → real-world learning.
Then repeat.
Here’s a peak at how we do it at Panoptic Bio: